Do I Have a Labral Tear? What You Need to Know About Treating This Common Ballet Injury

In fall 2012, New York City Ballet associate artistic director Wendy Whelan, then a company principal, was taking morning class when her foot slid out from under her, causing her to pull the very top of what felt like her right hamstring muscle. “It shocked me from the inside out,” she notes.
Whelan spent three months nursing her hamstring. But once she got back to performing, her right hip flexor began flaring up. “By the end of Nutcracker season, I could no longer bear standing in fifth position. I could not lift my right leg without severe pain,” she says. “I couldn’t imagine why or how this was suddenly becoming so debilitating.” A sonogram revealed a complex labral tear in Whelan’s hip.
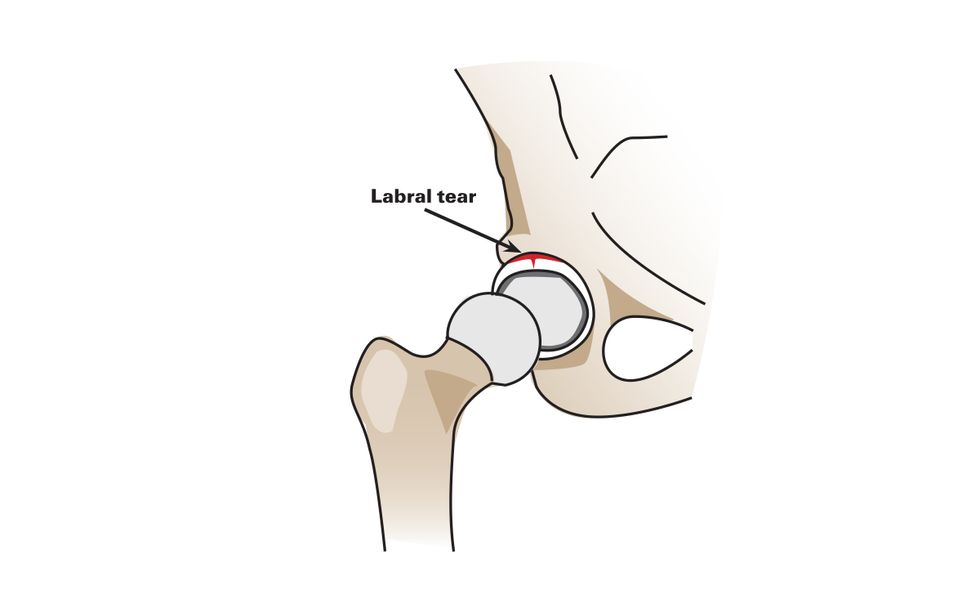
The labrum is a horseshoe-shaped band of cartilage that lines the acetabulum, or hip socket. The labrum’s soft tissue acts as a shock absorber; it also helps keep the ball of the femur securely positioned in the socket, provides stability and protects the joint surface. Whelan’s complex tear was more debilitating than most, but it’s important to understand the warning signs and varying treatment options available for this common and painful dance injury.
What Does It Feel Like?
Symptoms include a deep aching or burning sensation in the hip and groin area (sometimes the pain radiates to the back of the hip). Side extensions, like développés or grands battements, frequently worsen the pain and cause a flare-up. Often a retiré or fifth position can be irritating. Even nondance activities like climbing stairs, bending over, getting out of a car or walking may become difficult.
“Many dancers describe the pain like sandpaper in the joint,” notes Emily Becker, PT, DPT, a dance medicine physical therapist in Denver. You may also experience clicking or locking sensations when lifting or lowering the leg and feel limited range of motion and stiffness throughout the area. Sharp, stabbing sensations in the hip during quick movements can indicate a more significant tear.
Sometimes dancers can identify a slip or fall when the labrum tears abruptly. But often the pain comes on slowly due to progressive wear and tear of the joint. “There wasn’t a specific moment in which I knew something was wrong,” says Orlando Ballet dancer Isabella Mendez, who was a young trainee with the company when she was diagnosed with a labral tear. Instead, she gradually started feeling pain in her right hip during retirés and side extensions. “It eventually turned into constant pain,” says Mendez, who then saw an orthopedist.

Why Are Dancers So Prone to Them?
Dancers are prone to these tears because of the strain placed on their hip joints, and because labrums tend to dislike direct or rotational force. Many also discover that they have a rough edge or irregular shape along one or both of the hip bones called femoral acetabular impingement (FAI), which contributes to labral wear and tear.
“Hyperextension, in addition to doing oversplits, will weaken the hip ligaments,” says Becker, who adds that extreme stretching places stress on the labral tissue. “Forcing turnout on hips that are still developing will also strain the anterior capsule and create more instability of the joint,” she adds.
How Do You Treat It?
Once an orthopedist has diagnosed you with a labral tear, it’s important to know the treatment options available in order to decide which choice is best for you.
Conservative management, including massage, acupuncture, anti-inflammatory medication and physical therapy, is recommended first. Physical therapists work to strengthen the muscles surrounding the labrum, which frequently helps decrease pain and improve function and range of motion. Most doctors agree that once labral tissue is torn it’s not able to heal itself, but many dancers find relief from their symptoms with PT and can eventually return to dancing fully.
Unfortunately, depending on the location and severity of the tear, conservative treatment doesn’t always work. Whelan attempted many therapeutic procedures in search of relief, but eventually required labral reconstruction surgery. “When nonsurgical options have been exhausted and the dancer cannot perform due to pain, that’s when I would consider surgery,” says Dr. Andrew Wolff, an orthopaedic surgeon and athletic hip injury specialist with Washington Orthopaedics and Sports Medicine and an official physician for The Washington Ballet.
Currently, there are three arthroscopic procedures that can be performed if labral surgery is deemed necessary. (Wolff notes that recovery time is similar for each of these procedures. Dancers are advised to use crutches for about a month—usually it is less—and then to incorporate barre work after 8 to 12 weeks. High-level performance resumes after about six months.)
Debridement: The surgeon shaves off the ragged and torn areas of the labrum in order to limit further tearing and decrease pain.
Labral repair: The surgeon reattaches the torn portion of the labrum to the hip socket. This is most often done with small plastic pins/anchors and sutures.
Reconstruction: The surgeon removes the badly damaged, irreparable tissue, and the deficient labrum is replaced with an autograft (tissue from another area of the body) or allograft (tissue received from a tissue bank).
Many factors will determine which surgery is best. “These include the amount of damage to the labrum, the experience and skill level of the surgeon, and whether the athlete has failed a previous surgery,” says Wolff. “In my experience, athletes with severe labral damage or who have failed previous surgery almost always do better with a reconstruction.” There are currently only a handful of hip specialists in the U.S. who regularly perform labral reconstructions.
Though Mendez was able to complete her trainee year at Orlando Ballet, she was in so much pain that she elected to have debridement surgery once the season ended. Post-surgery, she took most of the summer off and began barre work after several weeks of physical therapy. Although she recovered, eventually becoming a full-fledged company member, she still performs hip-strengthening exercises. “I don’t have a lot of pain anymore, but sometimes my hip will remind me it won’t go a certain way or height.”
If you fear you have a labral tear, see your doctor—and keep in mind that many dancers are able to manage the injury and return to dancing fully. “Ballet is difficult and challenging, and one can’t help but experience occasional aches and pains,” says Whelan. “But learning how to listen to your body early on in your career can be extremely rewarding for it in the long run. We only have one body—we have to take the time to treat it well and check in with it thoroughly and thoughtfully each day.”
Try This Exercise for Stronger Hips

Emily Becker, PT, DPT, recommends this exercise to strengthen the hip extensors, hamstrings, glutes and core muscles. Conditioning these muscles will help dancers maintain healthy hips.
Stand in a parallel fourth position with your front leg in a demi-plié. The back leg will be standing on a resistance band (positioned under your arch). Hold both ends of the band in your hands with your elbows against your ribs and your forearms parallel to the floor.- In one motion, extend your arms forward and transfer all the weight onto your front foot while staying in plié and gently extending the back leg into a low arabesque.
- Return to parallel fourth. Practice 3 sets of 10 low arabesques.
Pay special attention to alignment so that your back does not arch in arabesque.
Think you have a labral tear? Don’t self-diagnose.
Other injuries, like bursitis and snapping hip syndrome (iliopsoas tendonitis), can cause similar discomfort. And according to Emily Becker, PT, DPT, stress fractures, a sports hernia, abductor strain or even ovarian cysts can also mimic labral tear symptoms. “It’s always best to see an orthopedic MD (or a physical therapist) to obtain a correct diagnosis and decide if any imaging is warranted,” says Becker.